Should I have my aneurysm clipped or coiled?
Understanding the differences between clipping and coiling for brain aneurysms and how to decide which treatment may be best for you.

You may be in the situation where doctors have recommended treatment for a brain aneurysm but two options have been offered: clipping (surgery) or coiling (endovascular treatment). This can be confusing, especially since each treatment has different pros and cons. To make the decision, it is best first to understand the two treatments in detail, as your own priorities may align more with one than the other.
Note that the information below is mainly applicable to unruptured aneurysms. If the aneurysm has recently ruptured then endovascular treatment is generally the first-line treatment unless it is not possible to undertake it. We mention the ISAT trial which involved ruptured aneurysms because this is one of a very few trials with systematic imaging follow-up that directly compared coiling and clipping.
What is clipping?
Clipping is a form of open surgery that has been used since the 20th century. It involves a craniotomy (opening the skull) to locate the aneurysm. Using a microscope, the surgeon places a small clip across the aneurysm’s neck, sealing it off from the blood vessel.
Can all aneurysms be treated with clipping?
Not quite all. Aneurysms in certain locations, especially in the posterior circulation (the arteries at the back of the brain), are much less commonly clipped as there is a higher risk of complications.
What are the benefits?
Clipping is an established therapy with an excellent chance of protecting the aneurysm.
What are the risks?
- Stroke in 5–15% of cases, which may cause weakness, speech, or vision problems. The lower end is more typical for straightforward anterior circulation aneurysms.
- Swelling around the brain at the site of the surgery, which can cause symptoms that are usually temporary.
- About 1% risk of severe brain injury or death.
- Rarely, seizures (epilepsy) or infection of the bone flap site.
- Temporary discomfort may include swelling and bruising of the face (sometimes enough to close the eyes for a few days), headaches, a sensation that the bone flap is moving (this is harmless and settles as healing progresses), and difficulty chewing or opening the mouth due to muscle recovery, which usually improves within six months.
- Recovery is usually longer than with endovascular treatment. On average, patients are in hospital for about a week after treatment of unruptured aneurysms, although this may vary. A period of recovery at home is also usually needed, with time off work typically required.
Can aneurysms recur after clipping?
Yes, although this is rare. In the ISAT trial, 6% of clipped aneurysms were incompletely occluded at follow-up. It is worth noting that recurrence rates for unruptured aneurysms are lower than this.
Can aneurysms bleed after clipping?
This is very rare but not impossible.
Are aneurysms monitored after clipping?
In the UK, aneurysms are usually not monitored with scans after clipping unless there is a particular concern.
What is coiling?
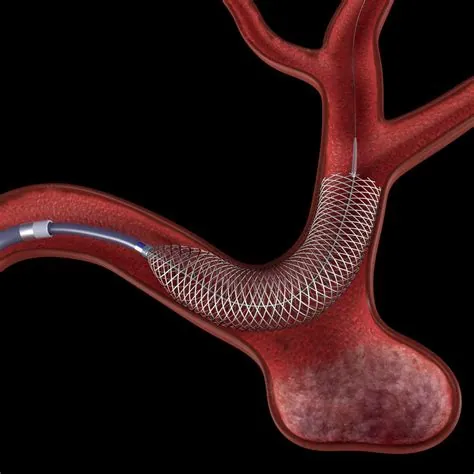
Coiling is a form of endovascular treatment developed to overcome some of the shortcomings of surgery. It is not a temporary treatment. The intention is to provide life-long protection against aneurysm rupture. A thin catheter is passed from the groin or wrist into the brain’s blood vessels. Platinum coils are placed into the aneurysm, blocking blood flow. Coiling is often combined with other techniques such as stents, flow diverters, or intrasaccular devices to make treatment safer and more effective.
Can all aneurysms be treated with endovascular treatment?
Almost all aneurysms can now be treated endovascularly, with rare exceptions.
What are the risks?
- Stroke in around 3–5% of cases due to rupture or blockage, usually lower than for surgery. In some series it can be slightly lower for elective, unruptured aneurysms.
- About 1% risk of severe brain injury or death.
- Rarely, vessel damage at the groin or wrist requiring surgery.
- Temporary symptoms such as soreness or oozing at the groin or wrist access site. Headaches may also occur in the days following the procedure.
- Recovery is usually rapid. Patients typically spend one night in hospital and go home the next day. Especially in older patients or those with health problems, coiling is often safer because recovery is easier.
Will I need to take life-long blood-thinning medication?
Simple coiling or intrasaccular devices generally do not require antiplatelet (blood-thinning) medication.
When a stent or flow diverter is used, antiplatelet medication is usually prescribed. This usually takes the form of two tablets: low-dose aspirin and a second tablet such as prasugrel (Efient), clopidogrel (Plavix), or ticagrelor (Brilinta). The second tablet is usually discontinued after about 6 months. The low-dose aspirin is usually continued for 1–2 years and then stopped, although rarely it is continued long-term. You will be advised whether this is needed before any procedure.
Can aneurysms recur after endovascular treatment?
Yes, although this is also uncommon. In the ISAT trial, 8% of coiled aneurysms were incompletely occluded at follow-up. If this happens, it is usually seen on scans and further endovascular treatment can be performed. It is worth noting that recurrence rates for unruptured aneurysms are lower than this, and modern treatments such as stents, flow diverters, and intrasaccular devices have further reduced recurrence rates.
Can aneurysms bleed after endovascular treatment?
As with clipping, this is extremely rare but not impossible.
Are aneurysms monitored after endovascular treatment?
Yes. Typically, follow-up scans are performed with MRA (magnetic resonance angiography, no radiation) or sometimes CTA or DSA (digital subtraction angiography). These are usually done for a few years and then stopped if the aneurysm is stable.
Key takeaways
- Both treatments are very effective, and the risk of bleeding afterwards is extremely low.
- Ultimately this is a personal decision, and the final choice depends on your own preferences and circumstances. We encourage you to talk to different specialists, and possibly also to those who have undergone treatment, to get as much information as you can before making the decision.
Full guide to brain aneurysms
Take control of your health with clear, expert information:
- What brain aneurysms are
- Diagnosis and treatment explained
- When to seek help
Aneurysm