Can you prevent brain aneurysms?
Are brain aneurysms inevitable or can you reduce your chances?

What causes aneurysms?
Unruptured intracranial aneurysms are found in about 3% of adults. Most aneurysms arise without a single identifiable cause. The vessel wall gradually weakens due to a mix of inherited and biological factors. Turbulent flow at arterial branch points and inflammation in the wall contribute to formation and growth.
At the same time, there are specific aneurysm types with clearer causes. For example, infectious aneurysms are due to infection of the vessel wall, dissecting aneurysms follow a tear in the inner lining, and traumatic pseudoaneurysms follow head injury.
What raises risk?
Non-modifiable factors. Age, female sex after the menopause, and family history matter. Risk is higher if you have two or more first-degree relatives with aneurysm or aneurysmal subarachnoid haemorrhage. Some conditions also raise risk, including autosomal dominant polycystic kidney disease, connective tissue disorders, and coarctation of the aorta.
Modifiable factors. Hypertension, smoking, heavy alcohol use, and stimulant drugs such as cocaine or amphetamines increase the chance of aneurysm formation and growth.
What can you do to reduce risk?
- Stop smoking. This is one of the most effective steps to lower formation and growth risk.
- Control blood pressure. Aim for good day-to-day control with lifestyle and prescribed medication.
- Moderate alcohol and avoid stimulants. Cut excess alcohol and avoid cocaine and amphetamines.
- General vascular health. Keep active, manage weight, and control diabetes and lipids where relevant. This supports healthier vessel walls. (Mechanism described in the aneurysm wall section.)
- Aspirin may be considered in selected cases. Some centres consider low-dose aspirin to reduce wall inflammation and the chance of growth or rupture, but this should be a clinician-led decision after weighing bleeding risks.
Should you be screened?
Population screening is not recommended because most aneurysms never rupture and screening does not prevent every bleed. Screening is usually offered if you have two or more first-degree relatives affected, or in certain conditions such as polycystic kidney disease or coarctation. If screening is needed, non-contrast time-of-flight MRA is preferred, typically starting around age 20 with repeat scans every 3 to 5 years until about 60 to 70, tailored to individual risk.
If an aneurysm is found
Finding an aneurysm is not the same as needing an operation. Most never cause symptoms and most never bleed. The annual rupture risk for typical incidental aneurysms is well under 1 in 400. The majority of incidental aneurysms are safely observed with risk-factor control and periodic imaging. Growth risk can be estimated with tools such as ELAPSS, and rupture risk with PHASES, to guide follow up and treatment decisions in a multidisciplinary meeting.
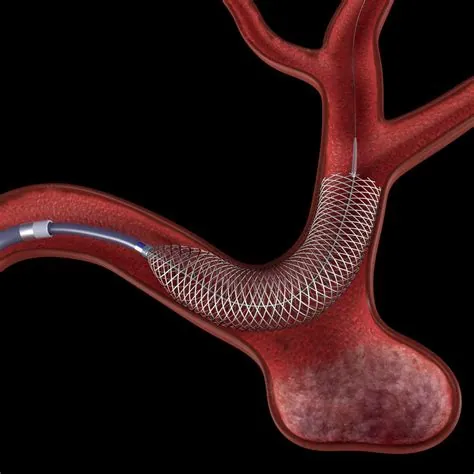
If treatment is advised, there are two main options: neurosurgical clipping and endovascular treatment such as coiling or flow diversion. Both are effective.Endovascular treatment is minimally invasive and is often associated with shorter hospital stays and quicker recovery than open surgery.
Finally, remember that the absolute risk of rupture in the general population is low. The incidence of aneurysmal subarachnoid haemorrhage is about 6 to 8 per 100,000 people per year. Focusing on blood pressure, smoking cessation and sensible screening where appropriate will do the most to reduce risk.
Key takeaways
- Short answer: you cannot prevent every aneurysm, but you can lower your risk and catch higher risk problems early.
- Aneurysms are present in about 3% of adults. Most never rupture.
- Most aneurysms are idiopathic in practice, but some types have defined causes such as infection, dissection and trauma.
- Reduce risk by stopping smoking, controlling blood pressure, moderating alcohol, avoiding stimulants and maintaining overall vascular health. Consider aspirin only on clinician advice.
- Most incidental aneurysms do not need treatment. When treatment is needed, both clipping and endovascular options are effective. Endovascular treatment is minimally invasive and often means a quicker recovery.
Full guide to brain aneurysms
Take control of your health with clear, expert information:
- What brain aneurysms are
- Diagnosis and treatment explained
- When to seek help
Aneurysm